
After the unfortunate event of having a limb amputated
two thirds of patients continue to feel the vivid sensation of a limb that is
no longer there. 50-80% of patients experience incredibly painful burning,
crushing or cramping in their phantom limb, leading many to depression and
suicide. The phenomenon of a phantom limb is one that usually diminishes in
time; but for some these phantom limbs stay present for years. Now a neuroscientist
from San Diego has come up with a novel way of relieving people of their
phantom.
V. S. Ramachandran’s first patient had his phantom
arm for 11 years, before which his arm was in a paralysed and sling after one
of the nerves was severed. After the amputation he had a phantom arm that was
still chronically painful and he believed to be paralysed. Ramachandran placed him
in front of a upright, side on mirror, and told him to place his left phantom
arm behind the mirror and his right normal hand in front of the mirror. He wriggled
his fingers on both hands and watched the reflection in the mirror. To his
surprise he could see, and for the first time in 11 years, feel his phantom arm
moving, and the pain was instantly reduced. After three weeks of daily
practicing with this mirror box, his phantom arm disappeared and there was a
remarkable reduction of pain.
{kind=link}
The fact that sensations of paralysis and pain were
perceived as being in the arm before and after the amputation is key to understanding what is going on here. Prior to the amputation the brain sent
signals to move the arm, but it received back sensory input that the arm would
not move. From this feedback the brain learnt the paralysis. So when the arm
was amputated and the brain was not receiving any input from it, the brain
assumed it was still paralysed.
However when in front of the mirror, the brain was
receiving a flurry of new mixed messages about the arm: the muscle cells in his
stump was telling the brain there was no arm, and in front of the mirror box
his motor command and vision told him there suddenly was a fully functioning
arm. Eventually the brain gave up on the arm, and learnt that it was just a
phantom.
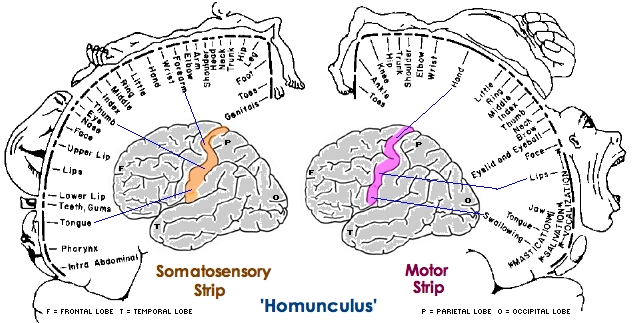
It all comes down to a part of the brain called the
somatosensory cortex which processes all tactile sensations received from the
skin. Sensory nerves from all of the skin have been mapped onto the
somatosensory cortex, and this enabled us to create a fetching map of sensory
input called Penfield Homunculi. Absence of sensory input from an arm for
example does not mean that part of the somatosensory cortex is necessarily idle
but continuously active, which is where the bizarre sensation of a phantom limb
comes from.
{kind=link}
The somatosensory complex tends to start reorganising
itself directly after amputation and for several years after, to try and
compensate for the loss of sensory input. Another patient of Ramachandran’s had
a painful left phantom arm, and he discovered that when touched on the right
side of his face he felt the sensation in his arm. They were able to map
sensations for each of his fingers onto his face. The Penfield Homunculi shows
the face representation is next to the hand representation, so it was concluded
likely that when the cortex received no sensory input from the arm, the area of
the cortex representing the face began to invade the hand region; creating the
misplaced sensations in the phantom limb.
Considering the plastic nature of the brain as
demonstrated here, it would be reasonable to say that in those who had a
phantom limb which disappeared in time, their brain accepts the visual
information of the limb not being there, and somatosensory complex reorganises
itself to not have an area for the limb which is no longer there.
An article I wrote for the second issue of QM Sci.
No comments:
Post a Comment